- Beyond colors, Blog Mawjoudin
- July 24, 2026
Beyond the Colors
HIV in Tunisia: The Silent Epidemic and the Challenges of an Unfinished Struggle
By Rihab Boukhayatia
According to updated data from the Ministry of Health released in December 2025, 7,700 people are living with HIV/AIDS in Tunisia.
The epidemic is spreading with an accelerated rate across North Africa, the Middle East, and within Tunisia itself. Fifteen years ago, around 70 new cases were reported annually; in recent years, however, that figure has risen sharply to between 420 and 430 new cases per year, according to Rim Abdelmalek, Professor of Infectious Diseases at La Rabta Hospital in Tunis.
This significant increase highlights the latent and underdiagnosed nature of this epidemic. Although HIV is a notifiable disease, it remains largely invisible among individuals who have not been tested.
Certain populations are particularly exposed, including men who have sex with men (MSM), sex workers, people who inject drugs (PWID), transgender individuals, and incarcerated persons, according to the National AIDS Control Programme (PNLS) of the Ministry of Health.
HIV prevalence rates within these groups are markedly higher than in the general population, ranging from 12% to 28%. They are estimated to be 12 times higher among sex workers, 13 times higher among transgender individuals, 19 times higher among MSM, and 28 times higher among people who inject drugs.
While this categorisation is necessary for tracking the epidemic and targeting public health interventions, it does not fully reflect the fluidity of human trajectories. A single individual may move among situations over time, sometimes combining multiple risk factors.
The PNLS report emphasises that “some individuals do not belong permanently to a single key population but may, intermittently or temporarily, integrate into another—for example, a person who injects drugs and occasionally engages in sex work, or a sex worker who uses injectable drugs.”
It also highlights the importance of considering gender dynamics among people who inject drugs. Women in this group are more exposed to HIV, partly due to their frequent involvement in sex work.
In addition to these key populations, the PNLS identifies groups deemed “vulnerable”: adolescents, young people, migrants, refugees, and other displaced individuals. Based on its biobehavioural survey, the PNLS notes that adolescents aged 15–19 and young adults aged 19–24 are among those most at risk of contracting HIV. Here, we are talking about a generation that is navigating social media, dating applications, and, in some cases, drug use.
HIV has long been perceived as a problem that only affects so-called vulnerable populations. However, it is now reaching the general population, including students, healthcare professionals, and others. The virus does not discriminate; it circulates silently through risky sexual behaviours that permeate all layers of society.
“In the course of our medical consultations, we are observing an increase in the number of young students and secondary school pupils, indicating a rejuvenation of the epidemic. However, we are also observing the emergence of cases among retirees and older adults,” explains Professor Abdelmalek.
She identifies multiple contributing factors behind the increase in people living with HIV, including drug use, chemsex, oral sex, and ulcerative sexually transmitted infections.
Chemsex is described by several civil society organisations working on HIV and STIs as a major concern. It involves the use of psychoactive substances during sexual activity. Often associated with disinhibition and pleasure, these substances are frequently addictive and include stimulants and euphoric drugs such as cathinones, cocaine, methamphetamine, and MDMA/ecstasy, sometimes combined with ketamine or GHB.
Chemsex sessions are characterised by repeated drug use and prolonged sexual activity lasting several hours or even days. These practices expose participants to multiple risks, including dependency, potentially fatal overdoses, and unprotected sex.
Sami, 38, has been living with HIV for three years. Prior to this change in his life, he did not imagine that he could be affected. Like many people in his generation, he believed that the virus only concerned others, but never himself. The shock was brutal and occurred in a still largely taboo context: chemsex.

At first, it was only about “spicing up” parties, he explains. He was unaware that the substances he consumed to stay awake, feel more confident, and lower inhibitions would make him extremely vulnerable. Sex and stimulants became intertwined, pushing the limits of both body and mind, with protective boundaries nearly erased. He vividly remembers the moment of testing: alone in a room, heart racing, trying to convince himself it was a false positive. The result, however, was clear and final—HIV-positive.
“I felt an urge to run away, to disappear, to punish myself. Then came the shame, the fear of judgement, and anxiety about telling my loved ones,” he recalls.
While Sami was aware of the risks and dismissed them, others—particularly young people—often lack sufficient knowledge about risky sexual practices. Among this population, misinformation and gaps in knowledge contribute significantly to the dissemination of HIV infections.
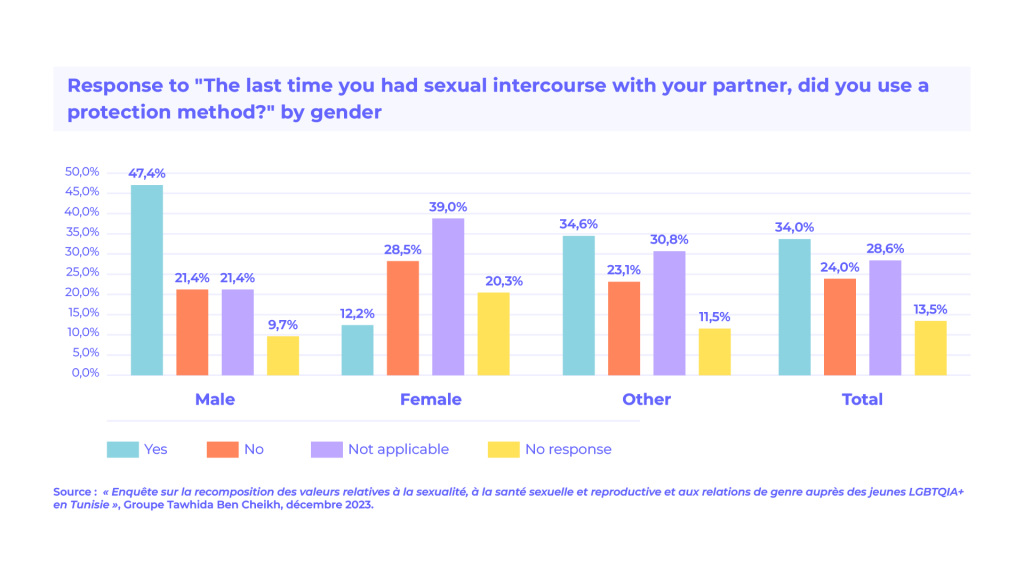
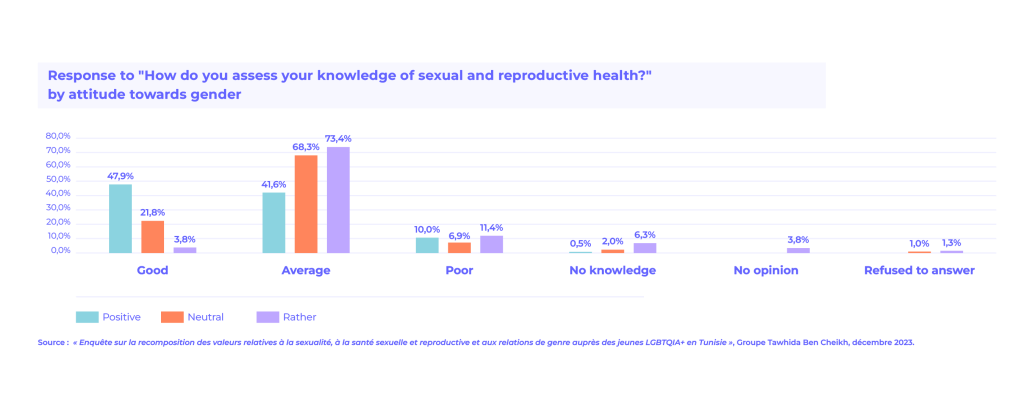
This is reflected in findings from a 2024 survey conducted by the Tawhida Ben Cheikh Group among 5,837 unmarried young people aged 18 to 29. The study reveals a structural deficit in knowledge related to sexual and reproductive health.
Fewer than half of male respondents and only slightly more than one tenth of female respondents reported using protection during their last sexual encounter. Knowledge of sexually transmitted infections remains limited, particularly among young men and LGBTQIA+ youth.
Women generally demonstrate higher levels of knowledge, but this also highlights persistent gender inequalities in access to information, the negotiation of sexual practices, and autonomy over one’s body.
Violence is another key driver of HIV risk, particularly among migrant populations. Sékou, a 28-year-old transgender woman from Guinea, was ostracised by her family and imprisoned due to her sexual orientation. She experienced blackmail and sexual violence in her home country before fleeing along a long migration route through Mali, Algeria, and Tunisia.
Upon her arrival in Tunis, she was hospitalised for an anal tear caused by these assaults. It was during this hospitalisation that she learned she was HIV-positive. Visibly weakened and emotionally distressed, Sékou recounts her story through tears. Her experience illustrates the extreme vulnerability of transgender migrants exposed to sexual violence, which significantly increases the risk of contracting HIV.
Testing: The First Line of Defence
The number of new HIV cases continues to rise annually. For Bahzed Welyeddine Fitouhi, President of the Tunisian Association for Health Education, this increase also reflects progress: expanded testing. “The more we test, the more cases we detect,” he explains.
He also highlights the expansion of target audiences through awareness campaigns that no longer focus solely on specific groups but address the broader population, including young people and previously undertested groups.
Innovative approaches—such as theatre, podcasts, and activism on social media—have helped reach the general public. As a result, there is now greater awareness of the true scale of the epidemic in Tunisia, which had previously been underestimated due to insufficient monitoring.
However, these improvements do not eliminate persistent barriers to testing, which mean that official figures are likely below real figures. Official data include only individuals who have been tested, diagnosed, and integrated into the healthcare system.
In theory, HIV testing is accessible to everyone in Tunisia. Free and anonymous testing centres exist in 24 locations across the country, and some hospital services also provide testing.
In practice, however, testing uptake remains low—far below the level required to effectively curb the epidemic. Why? Because stigma remains overwhelming.
Fear of judgement, social exclusion, or even retaliation within family or professional environments continues to discourage many individuals from getting tested.
Punitive laws surrounding certain sexual practices or activities further reinforce this climate of fear. A sex worker or a man who has sex with men, for instance, may fear being identified or stigmatised by the authorities or their own community.
“HIV is still associated with behaviours considered “taboo”, which fuels shame and prejudice. As a result, many people are unaware of their HIV status because they do not get tested, often due to stigma or fear,” Fitouhi explains.

To counter this, it is essential to create “safe spaces” for at-risk populations to encourage testing, notes Karam, a medical resident and volunteer with the Mawjoudin association.
“Even for simple testing, these spaces provide genuine listening and support, whether regarding romantic relationships, sexual issues, or questions of identity and gender orientation that are often misunderstood,” he tells us.
However, such spaces are becoming increasingly rare due to the recent restrictions on civic space. These restrictions have led, among other things, to the closure of the Mawjoudin association’s office, which previously provided support to vulnerable LGBTQIA+ individuals. The closure of such spaces significantly reduces access to testing and undermines the quality of care, which is essential for community trust and engagement.
Health authorities themselves recognise stigma and discrimination as “the main barriers to accessing HIV testing, prevention, and care services.” Approximately 65% of women aged 15 to 49 report having observed discriminatory attitudes related to HIV.
This ostracization leads to late diagnosis and delayed treatment. Individuals who are unaware of their HIV status risk transmitting the virus unknowingly and may experience progression to AIDS with preventable complications.
On a psychosocial level, late diagnosis can trigger anxiety, isolation, and depression, among other invisible yet deep effects. “Unfortunately, late diagnoses are still common. The main causes are lack of awareness of risk-taking, the belief that it only happens to others, lack of regular testing, fear of the unknown, and ignorance of symptoms,” adds Professor Abdelmalek.
Access to Treatment: Access to Treatment: An Uphill Struggle
Stigma also affects access to care. Medical management of PLHIV has improved significantly. Antiretroviral treatments are available free of charge and allow effective viral suppression, reducing both morbidity and transmission risk.
However, inequalities in access persist. Services are centralised in four university hospitals—in Tunis, Sfax, Sousse, and Monastir—creating geographical and financial burdens for individuals in interior regions. For example, a person living with HIV in Kasserine must travel long distances to receive treatment, which is particularly challenging given their health condition. Medication access is another issue. Souhaila Bensaid, President of the Tunisian Association for Positive Prevention (ATP+), reports recent shortages of essential medications in some hospital pharmacies. In addition, patients are sometimes simply redirected to distant facilities to obtain treatment.
Poor management is compounded by ongoing discrimination and breaches of confidentiality in healthcare settings, particularly among paramedical staff.
These issues These attitudes stem from a lack of knowledge and prejudice, unlike with the medical staff, which is more firmly rooted in scientific principles, points out the president of ATP+.
People living with HIV report that they are judged more harshly by nurses and healthcare workers, according to a survey by the Pasteur Institute entitled “The care of people living with HIV in healthcare settings: results of a qualitative survey.”
The survey also highlights serious breaches of disclosure protocols and medical confidentiality, as well as the disclosure of HIV status by paramedical staff in the near-total absence of any psychological support.
These are serious ethical and professional breaches. Such practices have profoundly detrimental consequences, not only for patients’ mental and physical health, but also expose them to major disruptions in their personal, family and social lives, which can even put them in danger, according to the authors of the aforementioned study.
In August 2025, the Ministry of Health issued a directive prohibiting the unnecessary mention of HIV status in non-medically justified documents.
This ministerial intervention followed observations that some healthcare institutions continued to display patients’ HIV status on bedside signs, transfer documents, and medical test requests, practices that violate confidentiality and contribute to stigma and discrimination.
These systemic issues contribute to the interruption of treatment, leading to patients being classified as “lost to follow-up.” For migrants, these challenges are compounded.
Sékou, for example, struggles to adhere to treatment due to racist behaviour from some healthcare staff. “Hostile stares, whispers, and dismissive expressions start as soon as I arrive,” she explains. Language barriers further complicate her access to care. Despite her fragile health, she approaches each medical visit with anxiety, even though it is essential for her survival.
Interruptions in care increase individual health risks and hinder efforts to control the epidemic.
Prevention: Structural Challenges and Social Urgency
The PNLS advocates for a “combined prevention” strategy, integrating behavioural, biomedical, and structural approaches. This includes condom promotion, HIV and STI testing, harm reduction strategies, and antiretroviral-based prevention, all within a framework grounded in social justice and human rights.
However, the implementation of this model faces significant challenges. The system suffers from administrative and financial fragility, directly and critically affecting the daily lives of people living with HIV, says Souhaila Bensaid.
The national programme is severely understaffed, with only one person managing all cases, which weighs heavy on access to treatment. PLHIV often face exhausting administrative procedures and costly travel among institutions to access minimal financial assistance (varying between 20 and 180 Tunisian dinars) or simply to obtain treatment.
The withdrawal of Global Fund support has worsened this situation of precariousness, including the loss of essential assistance such as milk and diapers for affected families. The most vulnerable households are thus left to their devices, explains the president of ATP+.
It also highlights the persistence of stigma within public administrations themselves, where disability-related priorities are no longer systematically upheld.
Responding to the emergency
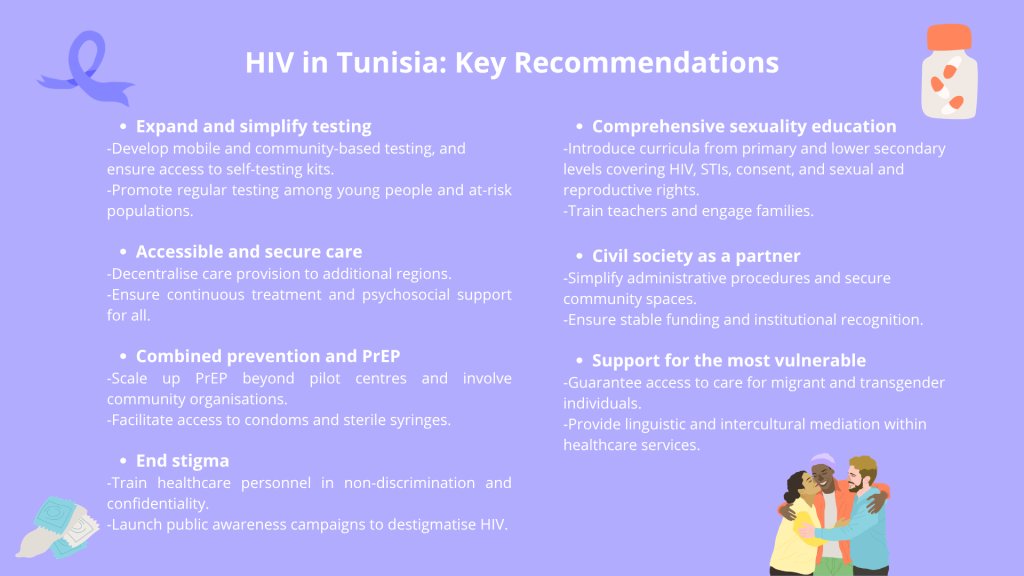
“Prevention is a central pillar in curbing the rise in new cases. It is essential to train healthcare professionals to integrate preventive approaches into their daily practice and to recognise indicative symptoms. Efforts must also be made to combat stigma and criminalisation, in order to enable effective intervention in certain sectors and among the most vulnerable populations. Promoting regular testing, encouraging the use of PrEP and condoms, ensuring access to single-use syringes without mandatory exchange schemes, strengthening drug policy responses, and providing better support to migrant populations so they are encouraged to seek care and receive appropriate treatment, these are all key priorities” argues Dr Rim Abdelmalek.
Prevention therefore requires a combined medical, educational, and social approach. From a medical perspective, current efforts rely largely on the use of PrEP.
Pre-exposure prophylaxis (PrEP) is a preventive antiretroviral treatment intended for HIV-negative individuals. It is widely recognised for its high level of effectiveness in preventing HIV infection following exposure to risk. It may be taken either daily or on an event-driven basis, according to a medically supervised regimen. Its prescription requires regular monitoring, including HIV and STI testing.
Despite its proven effectiveness, access to PrEP in Tunisia remains highly limited. It is still confined to a pilot phase and has not yet been integrated into a national prevention strategy. Reference centres are primarily located at Fattouma Bourguiba Hospital in Monastir and La Rabta Hospital in Tunis—an availability that falls far short of current needs.
Associations are not authorised to provide PrEP, a restriction that frustrates Souhaila Bensaid. “Offering PrEP exclusively within treatment centres is not conducive to uptake,” she notes, adding: “I fail to understand why associations are permitted to conduct testing but not to provide PrEP, given that testing is equally a sensitive and complex task.”
Limiting PrEP provision to hospital-based settings reduces both accessibility and acceptability among the populations most at risk, she adds. Even individuals who wish to access these services within said centres often encounter difficulties in securing appointments.
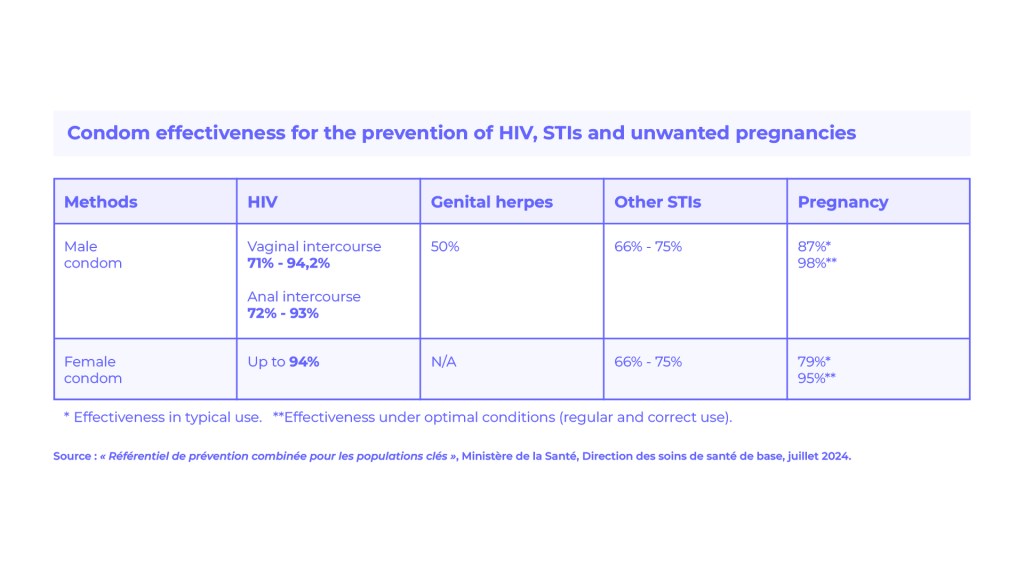
Beyond PrEP, access to condoms is also constrained. “Condom distribution has become problematic due to security concerns, particularly the risk of being associated with sex work, even during community-based events,” Karam laments.
According to the National AIDS Control Programme (PNLS), condom use among key populations remains low and does not exceed 60%, with significant disparities: from 46.7% among people who inject drugs to 58.3% among sex workers.
Young people, in particular, are left to navigate these issues with little to no support. As a cornerstone of HIV and STI prevention, comprehensive sexuality education has yet to be effectively implemented within Tunisia’s education system. As a result, young people are deprived of a holistic, scientifically grounded understanding of modes of transmission and prevention of HIV and STIs, as well as of consent, bodily autonomy, and sexual and reproductive rights.
This restrictive approach reinforces the taboo surrounding sexuality, obscures real risks, especially among adolescents and young adults, and creates fertile ground for misinformation.
However, there is clear public demand for sexuality education. A recent survey on mothers’ attitudes towards their children’s sexual education, conducted by the Tawhida Ben Cheikh Group and published in December 2025, found that a strong majority of mothers (81.3%) support the integration of sexuality education into school curricula. Support increases with educational attainment, ranging from 77.6% among non-schooled mothers to 87.6% among those with higher education.
Lower secondary school (collège) is the level most frequently identified for the introduction of such education (42.2%), while a significant proportion of mothers also consider primary school an appropriate starting point (26.4%), underscoring the importance of early awareness.
Despite this need and the public health urgency, the state continues to hesitate. In 2020, the Ministry of Education announced the introduction of sexuality education at primary level, yet this commitment has not been implemented.
Another key pillar of prevention is the fight against stigma. Stigma remains one of the principal barriers to prevention, discouraging individuals from seeking testing, adopting protective measures, or engaging with care. The criminalisation of same-sex relations, drug use, and prevailing social conservatism all contribute to the marginalisation of people living with HIV.
Civil society organisations working with these populations are likewise affected by repressive measures. Increasingly stringent administrative procedures and heightened security controls are hindering their activities. “Organisations are now required to navigate ever more complex procedures simply to continue their work,” regrets Souhaila Bensaid.
The civil society, however, holds significant strengths, particularly its proximity to key populations and its capacity for innovation through peer education and alternative forms of expression such as artivism.
Nonetheless, it faces considerable constraints: limited geographical coverage, unstable funding, and a lack of institutional recognition. It cannot replace the state, but must instead be regarded as a strategic partner, emphasises Bahzed Welyeddine Fitouhi.
HIV prevention in Tunisia continues to be constrained by persistent political barriers, despite the presence of strong medical expertise.
Without genuine collaboration between the state and civil society, and without a destigmatised and inclusive approach, prevention efforts will remain partial and ineffective, leaving key populations exposed to risks that are, in many cases, preventable.